-
expertise
integrity
results
Foot & Ankle
Orthopedic Surgeon
Limb Lengthening &
Deformity Correction -
Biography
I am a board certified orthopedic surgeon who graduated from Indiana University School of Medicine in 1999. My career at Henry Ford Hospital started with orthopedic residency which I completed in 2004. I have since completed two fellowships, the first in foot and ankle surgery at the University of Washington and the second in limb lengthening and deformity correction at the International Center for Limb Lengthening in Baltimore. The combination of these two fellowships makes me uniquely qualified to take care of the most complex of cases.
My goal is to provide each and every patient with the best available treatments that focuses on their individual circumstances and needs. I believe that patient education is the cornerstone of the patient-doctor relationship. Surgical intervention is utilized in cases where nonsurgical options (bracing, medication, physical therapy, activity modification, time) have not been successful or when surgery is simply the most predictable and reliable measure to achieve the best possible outcome.
-
Bunions
Bunions are quite common and often are associated with a positive family history. Most bunions do not cause enough discomfort to warrant surgery.
However, if surgery is indicated, it is important that the correct bunion procedure is done to minimize the chance of recurrence.
The case examples demonstrate the various procedures performed depending on the severity of the bunion.
Back -
Bunionette
This involves a prominence of the fifth metatarsal on the outer surface of the foot. This can cause pain with tight fitting shoe wear.
Surgical treatment helps to narrow the foot and relieve pressure.
Surgical correction is indicated when wide and accomodative shoes do not lead to resolution of symptoms.
Backcase examples
-
Plantar Fasciitis
Heel pain is one of the most common foot and ankle conditions that affects patients.
It is associated with prolonged standing, a tight Achilles tendon, and being overweight.
Fortunately, most patients respond to heel cups, stretching, night splints, formal physical therapy, and occaasional injections.
Surgical treatment is rarely indicated but can be helpful in the most resistant cases.
Back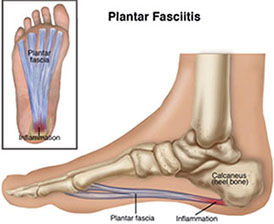
-
Hammer/clawtoes
Clawtoes are simply a more severe form of hammertoes which can also including overlapping of the toes.
They tend to be seen with bunions and be the result of tightly fitting shoes.
Nonsurgical treatment includes comfortable shoewear, padding and strapping.
Surgical treatment typically includes removal of the contracted joint and placement of an external pin. In less severe situations, the contracted joint can be released and pinned without removing the joint.
Backcase examples
-
Mortons Neuroma
This involves thickening of the nerve that can lead to burning type pain which is worse with shoewear.
Patients typically respond to a combination modified shoe wear, metatarsal pads, and infrequent injections.
Patients who do not respond well to injections may have been falsely dia\gnosed with a neuroma Ultrasound can help confirm the diagnosis in unclear cases.
Surgical removal of the nerve should be considered in patients whose pain persists despite appropriate treatment.
Back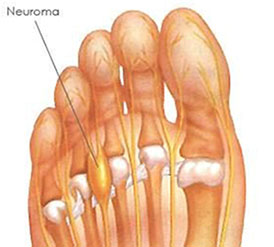
This diagram demonstrates thickening of the nerve leading to pain.
-
Flat feet
Flat feet are common and can be present as a child, the result of a traumatic injury, or age related.
Most patients do well with a combination of arch supports, antiinflammatories, physical therapy, as well as bracing or casting depending on the severity of symptoms.
Operative treatment is reserved for the most severe cases. The type of procedure would depend on the severity of the flat foot.
Moderate flat foot deformities tend to do well with osteotomies (bone cuts) and tendon transfer leading to realignment of the foot. More severe flat feet may require multiple osteotomies or fusion to adequately correct the foot alignment.The case examples demonstrate the various procedures performed depending on the severity of the flat foot.
Backcase examples
-
HIGH ARCHED FEET
Cavus feet tend to be stiff causing pain and can lead to ankle instability because of malalighment.
Peroneal tendonitis or tears can occur as well. Accomodative shoe inserts can be helpful as well as bracing in more severe cases.
Surgical treatment focuses on realigning the foot as well as treating associated tendon or ligament tears.
This may include osteotomies (bone cut), tendon lengthening, and tendon transfer to reblance the foot. Various joint fusions can be performed for the most severe deformities that can can not be adequately treated with joint sparing procedures.
Backcase examples
-
Midfoot arthritis
Arthritis of the midfoot can cause significant pain and debility. Anti-inflammatories as well as shoe inserts and rocker bottom shoes can be helpful.
When a large prominence is involved, it can be removed in order to allow for more comfortable shoewear and pressure reliefe on the nerve.
In more severe cases, a fusion can be done to relieve pain and enhance function.
Backcase examples
-
ARTHRITIS OF THE BIG TOE
Hallux rigidus is typically associated with a history of trauma but can also be associated with a long first metatarsal or an atypically shaped metatarsal head.
When painful, they are typically associated with large spurs that limit shoe wear. Accomodative shoe wear, anti-inflammatories, and injections can help treat pain.
Back -
Ankle Conditions
Ankle Arthritis
Causes for ankle arthritis include a history of multiple ankle sprains ...
Malalignment
Ankle and lower extremity malalignment causes increased ...
Ankle impingment
Spurs can develop as the result of ankle trauma.
Os trigonum
Posterior ankle pain secondary to an os trigonum can be related to ...
insertional achilles tendonitis
Pain at the insertion of the achilles tendon can be difficult to treat ...
Osteochondral lesions of the talus (OLTs)
OLTs result from severe ankle sprains and can be a cause ...
Achilles tendon rupture
The Achilles tendon is the largest tendon in the body and ...
Achilles tendonitis
Repetitive stress can lead to accumulation of microtears of ...
Peroneal tendon tears
Recurrent ankle sprains can cause peroneal tendon tears.
Ankle sprains
Ankle sprains are exceedingly common injuries whether related ...
Ankle instability
Tears of the lateral ankle ligaments can lead to an instability.
Peroneal tendon dislocation
The superior peroneal ...
-
Ankle Arthritis
Causes for ankle arthritis include a history of multiple ankle sprains, severe fractures, malalignment of the ankle/leg, inflammatory arthritis (rheumatoid arthritis, lupus, gout, etc.), as well as hemophilia. Nonoperative treatment focuses on anti-inflammatories, bracing, limited injections, and activity modification.
When these measures are not successful, surgical treatment involves joint sparing procedures like spur removal and realignment as well as ankle replacement and ankle fusion.
case examples
-
Malalignment
Ankle and lower extremity malalignment causes increased stress on the foot and ankle leading to pain and arthritis.
Nonoperative treatment measures like bracing, anti-inflammatories, activity modification, and selective injections can be helpful in less advanced cases.
Osteotomies (bone cuts) can help to restore alignment and improve lower extremity mechanics. This includes osteotomies to help restore alignment of the femur, knee, tibia, and ankle.
-
Ankle Impingment
Spurs can develop as the result of ankle trauma. These spurs can lead to pain and decreased ankle range of motion.
Removal of these spurs, whether arthroscopically or through a small incision can help relieve pain and increase range of motion.
Some patients with chronic ankle pain following an ankle sprain develop soft tissue impingement because of scar tissue formation in the ankle.
Most patients respond to targeted injections but ankle arthroscopy can be effective in more resistant cases.
-
Os trigonum
Posterior ankle pain secondary to an os trigonum can be related to an ankle injury.
Bracing, anti-inflammatories, activity modification, injections (ultrasound or x ray guided), and time can help relieve symptoms.
In patients with persistent pain, arthroscopic removal can be very helpful and allows for accelerated rehab and a quick return to activity.

Radiograph demonstrating an os trigonum inside the red circle.
-
insertional achilles tendonitis
Pain at the insertion of the achilles tendon can be difficult to treat nonoperatively since it is related to prominence of the calcaneus (Haglund's) as well as an insertional spur.
The combination of the spur and prominence of the calcaneus push against the achilles and cause trouble with shoe wear. Some patients improve with bracing, activity modification, anti-inflammatories, and time.
Injections are strongly discouraged as they can lead to further tendon degeneration and rupture. Surgical removal of the spur and calcaneal prominence as well debridement/repair of the Achilles can be effective in treating pain in resistant patients.
-
Osteochondral lesions of the talus (OLTs)
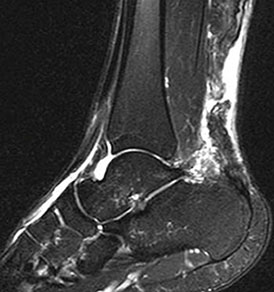
OLTs result from severe ankle sprains and can be a cause of persistent pain. They result from damage to the ankle joint cartilage. More chronic OLTs can be seen on x rays while smaller lesions and more acute lesions can be more easily identified on MRI.
It is important that a patient's pain correlate with the location of the OLT since many tend to not cause pain. When nonoperative treatment including anti-inflammatories, bracing, activity modification, time, and selective injections do not help, surgical treatment may be helpful.
Smaller OLTs can be treated arthroscopically by removing damaged cartilage to allow new cartilage to form. In patients who have recurrent pain after surgical treatment, cartilage plugs can be used to resurface the talus. Other grafts can be used as well (Denovo, Zimmer) for smaller recurrent lesions.
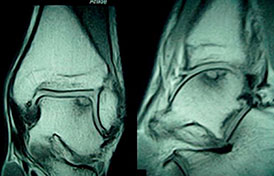
MRI of an osteochondral lesion of the talus
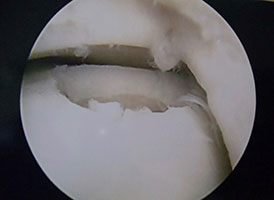
Arthroscopic image after the diseased cartilage has been removed
-
Achilles tendon rupture
The Achilles tendon is the largest tendon in the body and is subjected to a large ampunt of stress that could lead to rupture.
Nonoperative treatment is successful in most situations in appropriately selected patients.
Operative treatment can be helpful in younger high demand patients leading to a decrease in rerupture rates and more accelerated rehabilitiation.
I utilize an accelerated rehab protocol. After surgery, patients are allowed to progress to full weight bearing two weeks after surgery in a boot. The boot is discontinued after six weeks. Patients are never casted.

MRI and diagram showing Achilles tendon rupture
-
Achilles tendonitis
Repetitive stress can lead to accumulation of microtears of the achilles tendon and subsequent pain and dysfunction.
The majority of patients respond well to physical therapy, anti-inflammatories, activity modification, bracing, as well as nitroglycerin patches which helps increase blood flow to the tendon.
Surgical treatment typically includes achilles debridement, gastrocnemius lengthening to take stress off the tight achilles, and flexor halluces longus (fhl) tendon transfer to augment the function of the achilles tendon.
-
Ankle instability
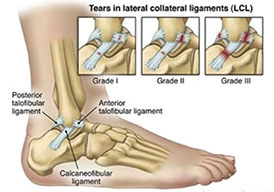
Tears of the lateral ankle ligaments (anterior talofibular and calcaneofibular) can lead to an instability.
When this persists despite nonoperative treatment, the ligaments can be reconstructed and retightened.
Patients are casted for a total of four weeks to allow for sufficient healing followed by physical therapy.
Surgery may also include tightening the ankle ligament (lateral collateral ligament), peroneal tendon repair, or surgery to address ankle cartilage damage.
Ankle sprain leading to ligament tears and possible instability especially with recurrent sprains

Extent of ligament injury depending on severity of the sprain
-
Peroneal tendon dislocation
The superior peroneal retinaculum can rupture as a result of an ankle sprain.
This leads to instability and dislocation of the peroneal tendons over the fibula.
Surgical treatment focuses on reattaching the superior peroneal retinaculum to the fibula.
-
Peroneal tendon tears
Recurrent ankle sprains can cause peroneal tendon tears.
Surgical repair is indicated in patients who have persistent pain despite nonoperative treatment measures.
Surgical repair allows patients to return to full activity when not previously possible.

-
Ankle sprains
Ankle sprains are exceedingly common injuries whether related to a slip and fall or a sports injury.
The overwhelming majority improve with nonoperative treatment including physical therapy, bracing, anti-inflammatories, activity modification, time, and targeted injections.
Patients unable to return to full activity despite aggressive nonoperative treatment may experience ankle instability, stiffness, nerve damage, cartilage damage (osteochondral lesions of the talus), as well as peroneal tendon tears or dislocation.
Ankle sprain leading to ligament tears and possible instability especially with recurrent sprains
Extent of ligament injury depending on severity of the sprain
-
Arthritis of the big toe (Hallux rigidus)

Hallux rigidus is typically associated with a history of trauma but can also be associated with a long first metatarsal or an atypically shaped metatarsal head. When painful, they are typically associated with large spurs that limit shoe wear. Accomodative shoe wear, anti-inflammatories, and injections can help treat pain.
-
Sports injuries
Achilles tendon rupture
The Achilles tendon is the largest tendon in the body and is subjected to a large ampunt of stress that could lead to rupture.
Achilles tendonitis
Repetitive stress can lead to accumulation of microtears of the achilles tendon and subsequent pain and dysfunction.
Stress fractures
These fractures occur from overuse and repetitive stress. Most stress fractures heal uneventfully.
Ankle sprains
Ankle sprains are exceedingly common injuries whether related to a slip and fall or a sports injury.
Ankle instability
Tears of the lateral ankle ligaments (anterior talofibular and calcaneofibular) can lead to an instability.
Peroneal tendon dislocation
The superior peroneal retinaculum can rupture as a result of an ankle sprain.
Peroneal tendon tears
Recurrent ankle sprains can cause peroneal tendon tears.
Os trigonum
Posterior ankle pain secondary to an os trigonum can be related to an ankle injury.
Osteochondral lesions of the talus (OLTs)
OLTs result from severe ankle sprains and can be a cause of persistent pain.
-
Stress fractures
These fractures occur from overuse and repetitive stress. Most stress fractures heal uneventfully.
MRI can aid in diagnosis as well as serial x rays. High risk stress fractures like the tibia, fifth metatarsal, navicular, and medial malleolus may respond to immobilization and external bone stimulator or may require surgery.
-
Foot Conditions
Bunions (Hallux valgus)
Bunions are quite common and often are associated with a positive family history.
Bunionette
This involves a prominence of the fifth metatarsal on the outer surface of the foot.
Plantar Fasciitis
Heel pain is one of the most common foot and ankle conditions that affects patients
Hammer/clawtoes
Clawtoes are simply a more severe form of hammertoes which can also including overlapping of the toes.
Mortons Neuroma
This involves thickening of the nerve that can lead to burning type pain which is worse with shoewear.
Flat feet
Flat feet are common and can be present as a child, the result of a traumatic injury, or age related.
High arched feet
Cavus feet tend to be stiff causing pain and can lead to ankle instability because of malalighment.
Midfoot arthritis
Arthritis of the midfoot can cause significant pain and debility.
Arthritis of the big toe
Hallux rigidus is typically associated with a history of trauma but can also be associated with a long first metatarsal or an atypically shaped metatarsal head.
-
limb lengthening
Limb length discrepancy can often lead to significant loss of function and disability.
Difference in overall leg lengths can result from congenital conditions as well as lower extremity fracture that lead to growth arrest in kids or fractures that heal in a shortened position in adults.
An internal lengthening nail (PRECISE nail, see links) or circular external fixator (Taylor Spatial Frame, see links) can be used depending on the specific needs of each patient.
case examples
-
fracture care
Fractures of the ankle and foot can be very serious and lead to long term impairment.
Recovery can often be prolonged because of the weight bearing nature of the ankle and foot.
Reestablishment of the overall alignment, early rehabilitation, and minimizing post operative complications is the key to obtaining the best outcome possible.
case examples
- ankle fracture (PDF)
- atypical calcaneus anterior process fracture (PDF)
- calcaneus fracture requiring fusion (PDF)
- tongue type calaneus fracture (PDF)
- lateral malleolus with syndesmotic fixation (PDF)
- lateral process talus fracture (PDF)
- severe lis franc (PDF)
- sports related lis franc (PDF)
- pilon fractuer with ankle dislocation (PDF)
- combined pilon and calcaneus fracture (PDF)
- high energy combined calcaneus and pilon fracture (PDF)
-
deformity correction
Lower extremity deformities lead to malalignment and increased stresses on the hip, knee, ankle, and foot. Most deformities are either congenital, developmental, posttraumatic, or secondary to neuropathy. The resulting malalignment can lead to altered walking, pain, and decreased levels of activity.
Realignment of the lower extremity helps to restore normal mechanics and forces across the hip knee, ankle, and foot. This can be accomplished by various techniques including plating, nailing, as well as Taylor Spatial frame (external fixator). In some deformities, a two stage approach can be used to correct the deformity with a Taylor Spatial frame followed by internal fixation (nail vs plate) that dramatically decreases the amount of time the external fixator is needed.
case examples
- Adult Blounts (knock kneed) (PDF)
- ankle arthritis malalignmeent ankle osteotomy (PDF)
- charcot midfoot charcot (PDF)
- chronic ankle fracture deformity (PDF)
- chronic tibial nonunion (PDF)
- dislocated choparts joint patient with clubfoot (PDF)
- distal tibia growth plate arrest with deformity (PDF)
- infected high tibial osteotomy (PDF)
- tibial malunion (PDF)
- tibial z deformity (PDF)
-
Ferras Zeni, M.D.
44633 Joy Rd., suite 200
Canton, MI 48187Phone: +1 (734) 255 0997